When Talk Therapy Hits a Wall: Why Traditional Therapy Often Isn't Enough for Trauma
Talk therapy hits a wall when insight can’t reach where trauma is actually stored. Cognitive, narrative-based approaches reach the brain regions that explain what happened — but trauma lives in the body’s alarm system, which responds to sensation, not words. That mismatch is why you can understand your story perfectly and still feel it in your body every day.
If you've spent years in therapy and can narrate your story perfectly — you know exactly what happened, you understand why it affected you, you can even explain your triggers to other people — but you're still waking up anxious, still flinching at a raised voice, still bracing for impact in moments that should feel safe... this article is for you.
You are not a therapy failure. You are not broken, unfixable, or "too damaged" for healing. What's far more likely is that you've been using a tool designed for one part of the brain to solve a problem stored in a completely different part. And that distinction changes everything.
Understanding why traditional talk therapy plateaus with trauma — and what actually reaches the places where traumatic memories live — can be the difference between spending another decade narrating your pain and finally moving through it.
Why Do You "Know" But Still "Feel"?
Trauma is stored not as narrative memory but as sensory and physiological experience—what van der Kolk (2014) calls “the body keeps the score.” When traditional talk therapy reaches a plateau, it’s often because the therapeutic approach addresses the cognitive story while the body’s alarm system remains unchanged.
There's a specific kind of exhaustion that brings people to my office after years — sometimes decades — of therapy. They sit down and within minutes, I hear some version of this: "I understand why I react this way. I can connect it to my childhood. My last therapist helped me see the pattern. But I'm still a mess. Nothing has actually changed in my body."
They still startle when their partner comes up behind them. They still shut down during conflict, watching themselves go blank even as they desperately want to stay present. They still feel a wave of dread wash over them when someone raises their voice or — worse — goes quiet. They still can't relax, even when they're objectively safe. The insight is there. The understanding is complete. The relief never comes.
And then they apologize. "I know I should be better by now. I've done so much therapy. I don't know what's wrong with me."
Here's what I tell them: Nothing is wrong with you. This isn't a failure of effort, motivation, or intelligence. It's a mismatch between the tool and the problem. Traditional talk therapy — including many forms of cognitive behavioral therapy (CBT) — works primarily through the prefrontal cortex, the part of your brain responsible for logic, language, analysis, and narrative. It's excellent at helping you understand your experience. But traumatic memories aren't stored there.
Where Does Trauma Actually Live in Your Body?
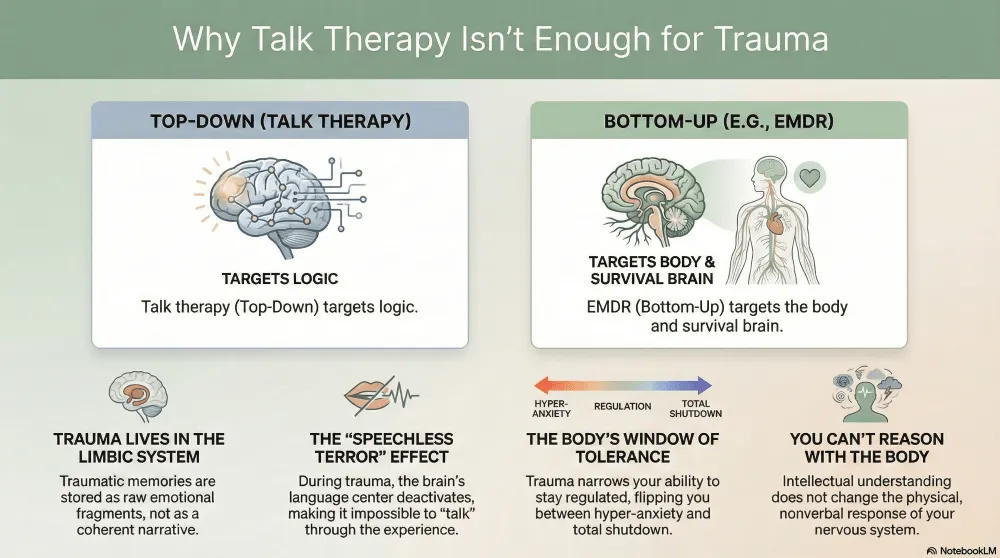
Dr. Bessel van der Kolk's groundbreaking research has shown us that traumatic memories are stored fundamentally differently than ordinary memories. When something overwhelming happens, the brain's normal filing system breaks down. The prefrontal cortex — your thinking, analyzing, narrating brain — goes partially offline. Broca's area, the brain's language center, deactivates. This is why so many trauma survivors describe "speechless terror" — the experience of feeling something intensely without being able to put words to it.
Instead of being processed, organized, and filed away as a coherent narrative (the way you remember what you had for dinner last Tuesday), traumatic memories get stuck in the limbic system — the brain's emotional and survival center. They remain as fragmented pieces: a flash of an image, a surge of emotion, a knot in the stomach, a sound that makes your heart race. These fragments don't come with timestamps. They don't feel like "the past." When they're activated, they feel like right now.
This is the core problem. People with active trauma responses have more reactive limbic systems, and — as van der Kolk's research established — ordinary talk psychotherapy does not decondition the limbic system. You can't reason your body out of reacting to stimuli that trigger a response at that level. The limbic system continues responding as if there are present dangers, regardless of what you intellectually understand.
Think of it like this: your thinking brain is fluent in language. Your limbic system speaks only in sensation, image, and survival impulse. Talk therapy is trying to have a conversation in English with a part of your brain that only understands the language of the body. No matter how eloquent the words, the message isn't landing where it needs to go.
"You can't reason the body out of reacting to stimuli that cause a reaction in the limbic system. Intellectual understanding does not change the nonverbal response."
Top-Down vs. Bottom-Up: Two Fundamentally Different Approaches
In the therapy world, we talk about "top-down" and "bottom-up" processing. Understanding this distinction can help you make sense of why your previous therapy was valuable — and why it wasn't enough.
Top-down processing starts with the thinking brain and works downward. This is what traditional talk therapy, CBT, and insight-oriented therapy do. You analyze your thoughts, challenge cognitive distortions, build narratives about your experience, and develop intellectual frameworks for understanding your reactions. This approach works beautifully for many challenges — depression rooted in thinking patterns, anxiety driven by catastrophic predictions, relationship skills that were never modeled. It's not a lesser form of therapy. It's simply designed for a different kind of problem.
Bottom-up processing starts with the body and the limbic system and works upward. Approaches like EMDR (Eye Movement Desensitization and Reprocessing) and somatic therapies access the places where traumatic memory is actually stored — in sensory fragments, body sensations, emotional surges, and survival responses. Instead of trying to think your way to a different feeling, bottom-up approaches help the nervous system complete the processing that was interrupted during the traumatic event.
Here's the metaphor I use: if trauma is a splinter lodged deep in muscle tissue, top-down therapy is like standing outside the body with a detailed diagram, explaining to the muscle why it hurts and where the splinter came from. Accurate. Perhaps helpful for context. But the splinter is still there, and the muscle is still in pain. Bottom-up therapy reaches in and removes it. Different tools. Different access points. Both have their place — but you can't extract a splinter with a lecture, no matter how insightful the lecture is.
Why Does Your Nervous System Have a Mind of Its Own?
Dr. Stephen Porges' polyvagal theory has given us a powerful framework for understanding why you can't simply think your way out of a trauma response. Your autonomic nervous system operates on three levels, each with its own logic — and it moves through them based on perceived safety, not rational analysis.
Here's what this looks like in real life: You're sitting across from your partner, who just asked a simple question — "Did you remember to pay the electric bill?" — and suddenly your heart is racing, your throat is tight, your hands are clenched, and every cell in your body is screaming DANGER even though your thinking brain knows this person loves you and is just asking about the electric bill. You watch yourself snap at them or go completely blank, and you can't stop it. That's your nervous system making decisions faster than your prefrontal cortex can intervene.
Three Levels of Your Nervous System's Response
- Ventral Vagal (Social Engagement): When you feel safe, your nervous system allows you to connect, communicate, think clearly, and be emotionally present. This is where your prefrontal cortex — and talk therapy — can do its best work.
- Sympathetic Activation (Fight or Flight): When your nervous system detects danger, it mobilizes you to fight or run. Heart rate increases, muscles tense, and your body floods with adrenaline. The thinking brain starts going offline. Gottman's research on couples calls this "flooding" — when heart rate exceeds 100 bpm, the capacity for listening, empathy, and creative problem-solving effectively shuts down.
- Dorsal Vagal (Shutdown/Collapse): When escape is impossible and the threat is overwhelming, your system shuts down entirely. This is the freeze, the numbness, the dissociation, the feeling of being "not here." Energy conservation replaces mobilization. You go flat.
Here's the critical piece: you cannot access your prefrontal cortex from a state of dorsal vagal shutdown. If your nervous system is frozen — which is exactly what happens when trauma is activated — the part of your brain that does the work in talk therapy is literally offline. Asking someone in dorsal shutdown to "think about this differently" or "use your coping skills" is like asking someone who is drowning to take notes on the water temperature. The system that would do that work has gone dark.
This is not weakness. This is not resistance. This is neurobiology. And it's exactly why years of excellent talk therapy can coexist with a body that still feels unsafe.
The Window of Tolerance: Why Trauma Survivors Live on the Edge (Understanding your attachment style helps explain why.)
Everyone has a window of tolerance — a zone where you can experience stress, feel emotions, process information, and still function. Within this window, you can reflect, connect with others, and engage with therapy productively. Above it, you're in hyperarousal: anxious, reactive, hypervigilant, unable to rest. Below it, you're in hypoarousal: numb, disconnected, shut down, unable to engage.
Trauma narrows this window — sometimes dramatically. Imagine that before trauma, your window was the width of a highway. Now it's the width of a balance beam, and you're trying to navigate daily life on it. A person whose window has been compressed by years of trauma may flip from hypervigilance to shutdown with very little provocation. They spend most of their time outside their window, which means they spend most of their time in a state where the prefrontal cortex is compromised and talk therapy can't fully land.
If you've ever sat in a therapy session understanding everything your therapist is saying while simultaneously feeling like your body is somewhere else entirely — like you're watching the conversation happen from behind a glass wall — that's the window of tolerance in action. Your thinking brain is engaged enough to follow the conversation. Your nervous system is not regulated enough to actually integrate the insight into lasting change.
How EMDR Reaches What Talk Therapy Can't
EMDR was developed by Dr. Francine Shapiro and has been extensively validated by research, earning the highest category of effectiveness from both the American Psychiatric Association and the Department of Veterans Affairs. But beyond the credentials, what matters is how it works differently.
Shapiro's Adaptive Information Processing model proposes that the brain has a natural system for processing and integrating experiences — similar to how the body heals a wound. When trauma occurs, this processing system gets blocked. The memory stays stuck in its raw, fragmented, emotionally charged form. EMDR uses bilateral stimulation — eye movements, tapping, or auditory tones — to reactivate this natural processing system and help the brain finish what it couldn't complete during the traumatic event.
During EMDR, clients focus on a specific traumatic memory — the image, the emotions, the body sensations, the negative beliefs attached to it — while simultaneously engaging in bilateral stimulation. This dual attention appears to activate the brain's information processing system in a way that allows fragmented, limbic-stored memories to be integrated into the brain's broader memory networks. What was stuck becomes unstuck. What felt like "right now" starts to feel like "that happened then."
What does this actually feel like in the moment? People often describe it as watching a movie that starts out vivid and terrifying, and then — as the processing continues — the images start to shift. The emotional intensity drains away. The body sensations release. New insights emerge that weren't accessible before. It's not forgetting. It's not minimizing. It's the nervous system finally completing the work it started years ago and couldn't finish.
What Changes After EMDR Processing
- Emotional charge reduces or resolves: The memory no longer triggers the same intensity of fear, shame, or helplessness.
- Negative beliefs shift: "I'm not safe" or "It was my fault" transforms into beliefs that reflect what you actually know to be true.
- Body sensations release: The knot in the stomach, the tension in the chest, the tightness in the throat — these physical markers of stored trauma resolve.
- The memory becomes narrative: What was fragmented sensory data becomes a coherent story you can tell without being hijacked by it.
- New responses become possible: Instead of reacting to triggers with the same rigid survival response, you develop what researchers call "response flexibility" — the ability to choose how you respond.
This is often what clients describe as the moment therapy finally "works" — not because they gained new insight, but because their nervous system caught up with what their thinking brain already knew.
Your Previous Therapy (Even if it didn't resolve the trauma bond.) Wasn't Wasted
If you're reading this and recognizing your own experience, I want to be clear about something: the therapy you've already done matters. The self-awareness you've built, the patterns you've identified, the relationship skills you've developed, the narrative you've constructed — none of that is wasted. In fact, it often makes EMDR processing more efficient. You've already done significant work on the cognitive and relational layers. What remains is the piece that talk therapy was never designed to reach.
Think of it as having done extensive architectural planning for a building renovation. The blueprints are brilliant. The vision is clear. But the foundation needs structural work that blueprints alone can't accomplish. EMDR is the structural intervention that works at the foundation level — the limbic system, the nervous system, the body — so that all the insight and skill-building you've already done can finally take hold.
"You're not a therapy failure. You were using the right tool for the wrong layer of the problem."
How Do You Know It's Time to Try a Different Approach?
Not everyone who's been in talk therapy needs EMDR. But if several of these resonate, a bottom-up approach may be the missing piece:
You Might Benefit from EMDR If:
- You can explain your trauma clearly but your body still reacts as though it's happening now
- You've gained significant insight in therapy but your triggers haven't actually decreased
- You feel "stuck" despite years of consistent therapeutic work
- You experience hypervigilance, startle responses, or chronic tension that cognitive strategies haven't resolved
- You dissociate or shut down during emotionally charged conversations
- You know intellectually that you're safe, but your nervous system doesn't seem to have gotten the message
- Conflict with your partner sends you into fight, flight, or freeze responses that feel disproportionate to the situation
What Should You Look For in an EMDR Therapist?
If you're considering EMDR, it's worth knowing that not all EMDR training is equivalent. Look for a therapist who has completed full EMDR training through an EMDRIA-approved program, who understands trauma and the nervous system beyond just the EMDR protocol, and who can integrate EMDR with other evidence-based approaches depending on your specific needs. A skilled EMDR therapist will also spend time building safety and stabilization before diving into reprocessing — this isn't a rush-to-the-trauma approach. The preparation work matters enormously, especially for people with complex trauma histories.
For couples where one or both partners carry trauma that's affecting the relationship, the intersection of EMDR with couples work can be particularly powerful. When your nervous system stops interpreting your partner's behavior through the lens of past danger, it creates space for genuine connection that wasn't accessible before.
You Deserve a Therapy That Reaches All of You (See also: When Healing Means Finding Who You Actually Are)
The fact that you've persisted in therapy despite not getting the results you hoped for says something important about you: you haven't given up on yourself. That persistence matters. It's a form of courage that often goes unrecognized — continuing to show up, continuing to try, even when the path forward isn't clear.
Trauma recovery isn't about talking more, analyzing harder, or trying to outthink your nervous system. It's about giving your brain and body the specific kind of support they need to complete the processing that got interrupted. When that happens — when the limbic system finally gets the help it's been waiting for — something shifts. The insight you've already gained transforms from something you know into something you feel. Your body catches up with your mind. The map and the territory finally align.
And that's where real healing lives — not in understanding what happened, but in your nervous system finally believing that it's over.
Disclaimer: This content is for educational purposes only and does not constitute medical advice or establish a therapeutic relationship. If you're experiencing a mental health crisis, please contact 988 (Suicide & Crisis Lifeline) or your local emergency services.
Continue reading in the Trauma recovery and healing series
- When Healing Means Finding Who You Actually Are — identity restoration as the next layer after nervous system safety.
- The Invisible Prison: Understanding Coercive Control — the framework that names why cognitive work alone can't reach embodied trauma.
- Is It Really Trauma Bonding? — the neurobiology that cognitive insight can see but can't reach.
- Understanding Your Attachment Style — attachment patterns written in the body before we have words.
- Glimmers — the daily practice that complements the intensive work.